
Conflicting Cascades: Comparing HIV treatment coverage estimates from UNAIDS and population-based surveys in Africa
On 20 November 2017, UNAIDS announced that 21 million people living with HIV are now accessing life-saving antiretroviral therapy (ART). For many, this is a landmark achievement and a promising sign that the Fast-Track targets can be met, and the world can end AIDS as a public health threat by 2030.
Others are more skeptical. At the 2016 International AIDS Conference in Durban, South Africa, a group or activists huddled in a dusty basement, questioning the validity of the then-tally of 17 million people on treatment. In a recent article published in the East African, AIDS Healthcare Foundation (AHF) called UNAIDS’ 21 million figure overly optimistic, inflated and inaccurate.
Organizations around the world have previously called for more transparency around the data, assumptions and methods that UNAIDS uses to generate treatment coverage estimates.
UNAIDS uses a combination of country-reported survey data and mathematical modelling to generate its statistics. The problem is – as AHF points out – the figures that countries report are not audited and the models are only as good as the data that goes into them.
One way to (crudely and rapidly) cross-reference UNAIDS’ treatment coverage estimates is to compare them to large country-level surveys. In 2016, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) conducted several population-based HIV impact assessments (PHIAs) in Malawi (“MPHIA”), Swaziland (“SHIMS II”), Zambia (“ZAMPHIA”) and Zimbabwe (“ZIMPHIA”). These surveys use a nationally-representative sample to estimate coverage of HIV testing, ART, viral suppression, among other indicators.
A rapid comparison between the PHIA survey results from Malawi, Zambia and Zimbabwe and the UNAIDS-reported treatment coverage estimates highlights some pretty significant discrepancies (Figure 1-3). Swaziland was excluded from the rapid analysis because UNAIDS is not yet reporting 2016 data for that country.
Note: each percentage in the graphs represents a proportion of the previous bar in the cascade. For this reason, some bars appear lower than others when the percentages are higher or the same value.
Figure 1: Comparison of UNAIDS and PHIA Treatment Cascades in Malawi (2016)
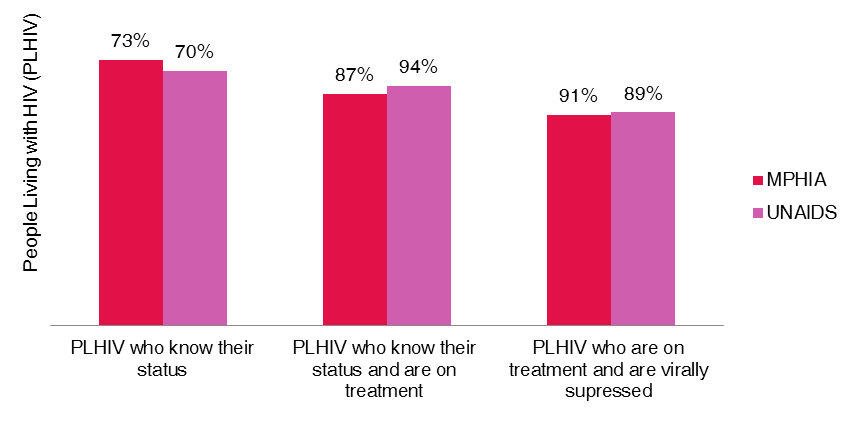
Figure 2: Comparison of UNAIDS and PHIA Treatment Cascades in Zambia (2016)
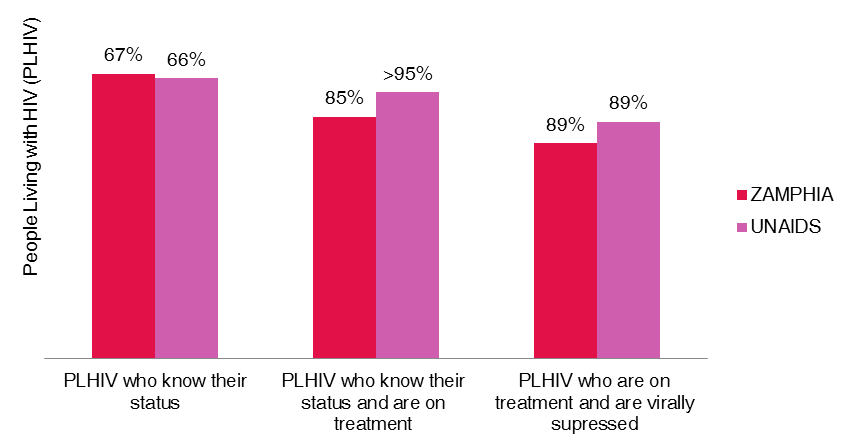
Figure 3: Comparison of UNAIDS and PHIA Treatment Cascades in Zimbabwe (2016)
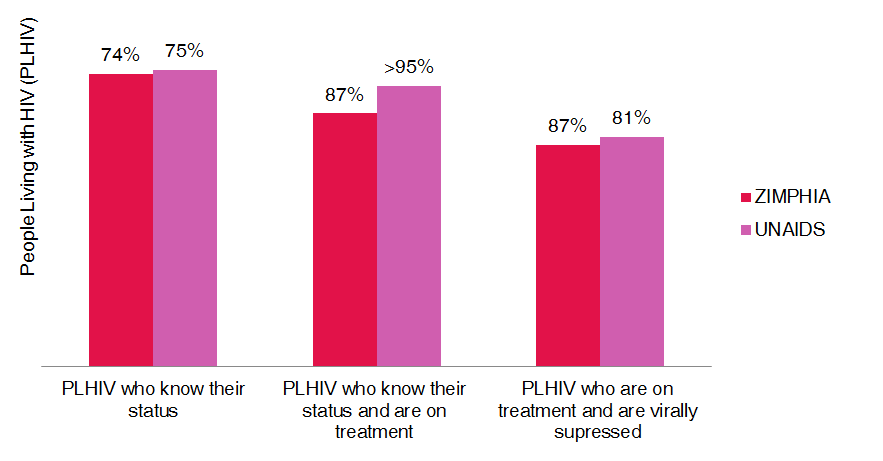
In all three countries, the UNAIDS estimates for HIV treatment coverage are higher than the survey data. The difference is most pronounced in Zambia, where the UNAIDS estimate is more than 10% higher than the ZAMPHIA survey result. In real numbers, UNAIDS estimates suggest that 181,210 more people living with HIV are accessing treatment than the population-based surveys found (22,900 more in Malawi, 69,000 more in Zambia, and 89,310 more in Zimbabwe).
The target for all countries around the world is to achieve 90-90-90 by 2020: By 2020, 90% of all people living with HIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy, and 90% of all people receiving antiretroviral therapy will have viral suppression.
UNAIDS estimates suggest that the second 90 has been achieved in Malawi, Zambia and Zimbabwe, whereas the PHIA data shows there is still further to go.
It is difficult to understand where the differences stem from, especially since UNAIDS uses the PHIA data from these countries as the numerator when estimating the proportion of people living with HIV who know their status. It uses Spectrum estimates as the denominator. Data sources and assumptions for the next two indicators in the cascade – treatment coverage and viral suppression – are not given.
Regardless of the reason for these conflicting cascades, they certainly have implications for funding, policy-making, and implementation at the country level. Planning for procurement and supply chain management of drugs depends on reliable estimates. Consensus on those estimates is also important for a harmonized multi-stakeholder response.
ICASO joins other civil society organizations in calling for greater transparency around how UNAIDS treatment coverage estimates are calculated.
By Gemma Oberth
11 December 2017